Physiotherapy Oakville : Glen Abbey Physiotherapy Shoulder Injuries, Types and Treatment Options in Oakville
Glen Abbey Physiotherapy treats all kinds of shoulder injuries. From slips and falls to baseball pitchers our physio team have treated all types of shoulder injuries in our Oakville clinic. Shoulder injuries can be caused by some of the most mundane events; computer posture, sleeping position, carrying your children or even walking the dog. Some of our physio patients have cool stories like dragon slaying, beer league hockey championship goals or watering planter boxes 😉 But most shoulder patients have nothing super cool that causes their shoulder pain.
Shoulder injuries can be broken down to 4 basic types 1. Rotator Cuff Injuries, 2. Labral Tears, 3. Bicipital Tenosynovitis and 4. Subacromial Impingement. The majority of our physiotherapy patients have some sort of rotator cuff injury with limited and painful range of motion. Their shoulder could hurt with pouring coffee or sleeping on their shoulder. They may or may not have a numbness down the injured arm. The symptoms of shoulder injuries are endless, let our Oakville Physiotherapist treat diagnose you and give you the treatment you need.
Move to: Rotator Cuff Injury
Move to: Labral Injury
Move to: Biceps Tendon Injury
Move to: Treatment for Shoulder Injury
Move to: Shockwave Treatment Oakville For Shoulder
Move to: Acupuncture Treatment Oakville For Shoulder
Rotator Cuff Injury
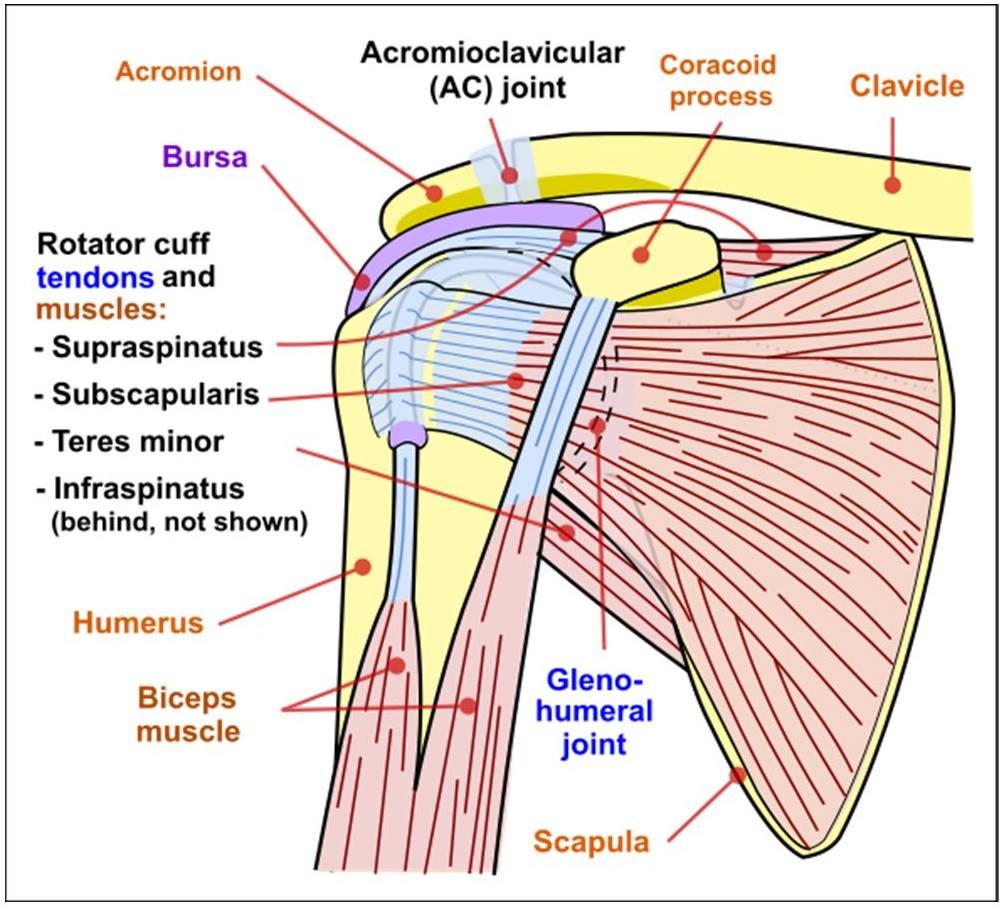
The Rotator Cuff is a combination of 4 muscles. Two internally rotate your shoulder, or win and arm wrestling fight and two externally rotate your shoulder or lose and arm wrestling fight. Injuries of the rotator cuff can occur from overuse, slips and falls and even sleeping positions. 50% of the patients we treat for rotator cuff pain have no specific reasons for their injury. The one common occurrence with these patients is sleeping with your arm above your head. So if you or a loved one are suffering from annoying shoulder pain and you sleep with your arm under your pillow, stop that ASAP!
The internal rotators are the supraspinatus and the teres minor. The vast majority of rotator cuff injuries are due to a supraspinatus issue. If you have pain throwing a ball or even lifting your arm up your side this is most likely due to a supraspinatus injury. There are usually four types of rotator cuff injury;
- Sprain/Strain
2. Tear
3. Tendinitis
4. Tendinosis
Learn more about rotator cuff injuries here
Rotator Cuff Strain
A Rotator Cuff Strain most commonly presents as shoulder pain with limited range of motion. With consistent treatment, there should be significant improvement in 6 to 10 visits. Strains can be caused by everything from overhead works, falls on ice, weekend warriors trying too hard to impress their wives during beer league baseball or sleeping awkwardly. The impairment experienced could be minimal to overwhelming pain. An ultrasound or MRI are used to confirm the injury, if the results come back negative (as in nothing found) the injury is most likely a strain of the rotator cuff muscle. Treatment and at-home exercises will be given and near full restoration of range of motion with limited pain should be noted in 2 to 4 weeks of treatment. Most often, our physiotherapists will treat conservatively, and only request imaging if the pain is not responsive to treatment.
Rotator Cuff Muscle Tear
A rotator cuff tear can be more complex to treat then a sprain. Tears range from tiny to complete, or more formally partial thickness to full thickness. The majority of rotator cuff tears are due to a repetitive shoulder movement, a yank or a slip and fall. Most patients do not feel the tear happen and present with the same symptoms as a sprain. The story can get even more muddled, because some tears happen over time due to repetitive stress. Signs and symptoms like limited range of motion, painful shoulder arc movements and pain with certain, usually mundane, shoulder motions, such as pouring coffee or putting a seatbelt on are common. Treatment for a rotator cuff tear mirrors that of a sprain/strain but a tear will take longer to heal. The tear will be confirmed with an ultrasound or a MRI. In most cases, if the patient does not have an ultrasound of their shoulder we will treat the patient. If the symptoms don’t decrease or the physiotherapist does not see the results they expect, they will ask their Medical Doctor for a visualization of the patients shoulder.
Rotator Cuff Tendinitis
Shoulder Tendinitis is the most common confirmed injury at our Oakville physiotherapy clinic. This will be confirmed with either an ultrasound or an MRI. Tendinitis is inflammation of a tendon or area around the tendon. Basically, some type of swelling is present. Once again, symptoms and presentation mirrors that of a sprain or a tear. In most cases patients with tendinitis will feel less pain and have increased range of motion with Advil or prescription NSAIDS. You do not need a cortisone injection with supraspinatus tendinitis, at least not right away. Tendinitis, like a tear, will take 4 to 8 weeks to improve with treatment. At that time, if the shoulder is not 80% better, our physiotherapist would suggest seeking further medical attention and the possibility of a cortisone shot. This would be after the Ultrasound or MRI confirmation of the Tendinitis, as mentioned above. It is ignorant to say a patient has shoulder tendinitis when it mirrors so many other injuries.
There is a subcategory of tendinitis that involves calcifications developing within the tendon. Calcific tendinitis is not well understood, but it has been proposed that it is caused by poor blood supply to the tendon, aging of the tendon, or delayed healing of tendon injuries. Instead of the body repairing the tendon with tendon fibers, it uses bone instead. It’s like the little pig who had his straw house blow down by the big bad wolf decided to rebuild with bricks from the neighboring pig’s house. Unlike most other shoulder injuries, calcific tendinitis can be seen on an x-ray and an ultrasound. Pain and symptoms associated with calcific tendinitis are the same as seen with regular tendinitis.
A Bunch of great Rotator Cuff exercises and videos can be found here
Shoulder Tendinosis
Shoulder Tendinosis has become more common over the last 2 to 3 years. The physiotherapists at our Oakville clinic are not sure if its just more prevalent in the population or the radiologists have altered their diagnostic approach to ultrasounds and shoulder tendinosis. First and foremost there is a huge difference between tendinitis and tendinosis. As noted above tendinitis is swelling and tendinosis is a cellular change WITHOUT any swelling. Our physiotherapists are amazed how many patients they get who have been given Naproxen or other NSAIDS (for inflammation) who have confirmed tendinosis. Literally, the oxford definition says there is no swelling, but a cellular change. The physiotherapy community is unsure why the tendinosis gets started or why it is present. In most cases it is thought to be a degeneration of a tendon from a previous injury. Shoulder Tendinosis, in most circumstances is the most difficult to treat. Pain patters will be all over the place. One day range of motion will be fine, 2 days later your shoulder will hurt and be limited movement with little to no aggravating factors.
Bicipital Tenosynovitis and Shoulder Pain
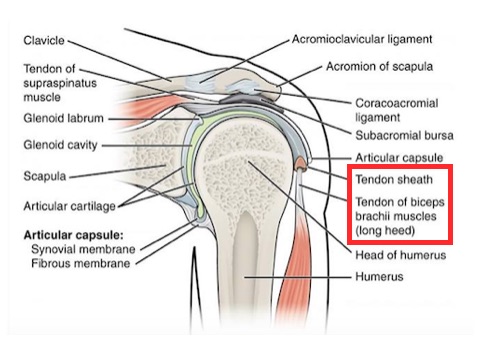
What on earth is tenosynovitis? Let us tell you. Tenosynovitis refers to a swelling/inflammation of the sheath of the biceps tendon. How is that different than a regular tendonitis? It’s the sheath. The sheath is a protective covering around the top of the bicep tendon and inside the sheath is a fluid that keeps the tendon lubricated and helps them slide with as little friction as possible. Many small tears that have accumulated over the years, or an acute trauma to the bicep itself can cause the inflammation of the tendon sheath. Repetitive use, prolonged use, heavy pushing/pulling/lifting are all risk factors for developing this specific inflammation. Symptoms include shoulder stiffness, limited and painful range of motion (especially reaching across the body), swelling and tenderness at the front of the shoulder and painful lifting.
Subacromial Impingement of the Shoulder
One of the more complex diagnoses of the shoulder is impingement. It is also one of the most common, some researchers say it can account for up to 65% of shoulder pain! By definition, this syndrome involves the ‘pinching’ of certain structures of the shoulder between two bony landmarks; the acromion and the arm bone. These structures that get pinched include the supraspinatus tendon and the subacromial bursa. A lot of important, pain-generating structures run through the small space between the bones of the shoulder/arm, and so when this space narrows it can cause all kinds of problems. This can be due to a degeneration of some shoulder muscles that allow for the bones to ride too close together, or due a specific configuration of the bony structures that make the pinching more likely. Our physiotherapists are highly trained to complete specific tests to determine whether or not your shoulder pain is caused by impingement.
Pain from this condition is usually described in a more general way, and is felt at the front of the shoulder. Pain may increase at night, or when laying down at the end of the day. This is because when you take gravity out of the equation, the tendons and/or bursa that have been getting pinched are un-pinched when the shoulder isn’t hanging, but are then allowed to swell and become inflamed. Range of motion, and pain with overhead activities can be extremely problematic.
Click HERE for Rotator Cuff Exercises
Oakville Physiotherapy Treatment for Shoulder Pain and Rotator Cuff Injuries
Treatment from our Oakville Physio team for shoulder pain and rotator cuff injures is not a one meets all criteria. Each patient is individually assessed and a game plan is developed for the characteristics of pain and shoulder symptoms on a case by case basis. Some shoulder injury patients who have identical ultrasound reports will display drastically different symptoms and their treatment plan will be tailored to their personal injury. In most cases treatment will include IFC, Active Release Therapy, Range of Motion Exercises, Shoulder strengthening exercises and at home icing and educational instructions. Some, more tedious shoulder injuries will need the help of shockwave therapy treatment or Acupuncture provided by Dr. Jenn.
IFC treatment
by our physiotherapy team in Oakville consists of 4 suction cup applicator pads placed in strategic positions around the shoulder. The current is then increased to just below painful. The patient will feel a deep tissue massage throughout their entire shoulder. The IFC treatment will help with pain relief, increase blood flow, decrease swelling and prime the shoulder for the next step in treatment. At this point a heat or ice pack could be added depending on the patients presentation of shoulder pain

Active Release Therapy
or Muscle Release is usually performed after the IFC machine has increased blood flow to the shoulder for 10 to 15 minutes. We are not gonna lie. ART can be painful , especially when done right. The Phyiso or Athletic therapist will place their thumb into different pressure points of your shoulder then move your shoulder through different ranges of motion to stimulate blood flow and break up muscle adhesion that are most likely the cause of your pain. They will make 5 – 10 passes and treat as many individual points as needed. More about ART here.
Basic Range of Motion Exercises
will be performed on site to help the patient relearn how and where their shoulder biomechanics should be moving. Some patients will be extremely limited in their range of motion and very little active treatment will be performed. Others will have great range of motion and our Oakville physio team will ensure that they are moving with the proper biomechanics.
Rotator Cuff Exercises
will be taught by our physio team onsite once the shoulder is moving better. We feel there is no point in trying to change the biomechanics of an injured shoulder while the tissue is still healing. Once the shoulder treating team sees fit. They will go over the phases of rotator cuff exercise prescribed by the physiotherapist. The patient will be encouraged to perform these exercises at home for 10 to 15 minutes a day.
Shockwave therapy
for rotator cuff injuries can be the saving grace chronic patients have been searching for. Shockwave Therapy uses a pneumatic gun with a bullet in chamber to break up scar tissue and improve blood flow and range of motion. The treatment needs to be on the edge of painful to work its best. The physiotherapy team will locate the area of dysfunction in the muscles of the shoulder and apply the shockwave gun to those areas. shockwave treatment for rotator cuff injuries in oakville will last between 2 and 3 minutes and most patients should feel a significant improvement after their first visit. More about shockwave therapy here.

Acupuncture treatment for shoulder injuries
Acupuncture is an extremely effective treatment option for shoulder pain. Whether the pain is caused by tendonitis, impingement or muscle strains, acupuncture can help. Acupuncture treatment for the shoulder typically involves the insertion of 5-12 needles along the spine and directly into the shoulder muscles. The needles stimulate blood flow to areas that need to be nourished, and helps to reduce the nerve irritation responsible for pain. One reason acupuncture is so effective is because the needles can reach parts of the muscles/tendons that a therapist’s hands can’t reach. Acupuncture is not painful, and typically yields quick and long lasting results. More about acupuncture for shoulder pain here.
Oakville Physiotherapy: Labral Tears of the Shoulder
What is the labrum of the shoulder ?
The labrum of your glenohumeral aka shoulder joint is what helps the ball and socket aspect of your shoulder stay together. Think of your labrum as a ring around the edge of the socket that helps the ball articulate or move better. Labral tears can actually be very common amongst baseball players and other sports involving the throwing motion such as javelin or football. The most common type of labral tear we see here at Glen Abbey Physiotherapy is called a SLAP lesion, although there are numerous other types of labrum tears which may occur. The SLAP lesion makes up the majority.
What is a SLAP lesion?
SLAP stands for superior labrum anterior and posterior. So essentially, a SLAP lesion is when you tear the top part of the labrum from front to back. SLAP lesions can be classified into Type 1-4 (1 being the most minor and 4 being the most major). Type 1 SLAP lesions are simply a small fray or tear occurring on the top part of the labrum. If you imagined the labrum like a clock, the ‘superior’ part of the labrum would be around 12 o’clock. These can usually be managed with conservative treatment by your Oakville Physiotherapy team. Type 2 Lesions are the most common and are usually associated with a dislocation. These lesions create a full detachment of the labrum and glenoid, therefore they are no longer attached and usually require surgical intervention. You Oakville Physiotherapy team at Glen Abbey would begin would rehab process the following weeks after surgery. Type 3 lesions are known as ‘bucket-handle’ tears. This is when the labrum tears off of the glenoid. Imagine if you could peel off the numbers 11, 12 and 1 on a clock, this flap is what the bucket-handle is. Most patients will complain of locking, popping or clunking of their shoulder because of the movement of this flap. Lastly, a type 4 lesion involves a tear to the labrum at 12 o’clock which also extends higher up into the tendon of the bicep muscle. These lesions are managed surgically and require what is known as a bicep tendinosis which is a surgical anchor of the bicep tendon back to the top component of the labrum.
Learn more about Shoulder Labral Tears here
Common Causes of a SLAP lesion
A SLAP lesion can be caused by a number of different mechanisms, but a few of the more common ones pertaining to baseball are as follows: falling on an outstretched arm, repetitive throwing and over extension of the shoulder. Examples of these are when a player may dive forward for a ball with a reached out arm or quickly reaching behind you to tag a base runner out. Any positional player could be susceptible to these mechanisms although pitchers tend to be the most common position related to these injuries seen at our Oakville physiotherapy clinic.
Signs and Symptoms of a SLAP lesion
The most common symptom across the board for SLAP lesions is intermittent pain; particularly with overhead movements. Patient’s will often also report painful popping or clicking with shoulder movement, decreased shoulder internal rotation, difficulty lying on that side and decreased shoulder strength and endurance. As a baseball player you may notice you cannot throw the ball as hard or as accurately as you used to be able to, or just that it causes you a lot of pain to do so. In baseball pitchers this is often referred to as a “dead arm”. Keep in mind these signs and symptoms overlap with other shoulder injuries, so make sure to come see us at Glen Abbey Physiotherapy so we can accurately diagnose your injury.
Diagnosing a SLAP lesion
Through both talking to you and performing a physical examination, our physiotherapists will have a good idea of whether or not you may have a SLAP lesion. We will perform a series of orthopedic testing, strength testing, length tension testing of both contractile and inert structures to get the best overall picture of the structures of your arm and which may be impaired from your injury. Imaging techniques such as an MRI with contrast may also be helpful to further confirm the diagnosis.
Treatment for SLAP lesions
Here at Glen Abbey Physiotherapy our team works around the clock to get you better. We utilize a full approach to help you achieve your goals and get you back to playing your sport and returning to your activities of daily living. Our team will introduce both passive, active and active assisted range of motion techniques to help you achieve the range of motion you need to get back to throwing or your regular hobbies and interests. We will introduce strengthening exercises progressively. Starting from isometric (non-movement) strengthening, to isotonic (moving) strengthening particularly focusing on your external rotation, abduction and flexion musculature to help you regain the power in the throwing and overhead motions. Although this all sounds easy, there may be times where pain may limit your movements, our team will utilize a series of modalities to help reduce your pain and discomfort throughout your treatment sessions. Finally, to restore end range motion and make sure the glenohumeral joint is articulating and moving in the proper motion, we will use manual therapy, mobilizations and soft tissue massage to help restore your shoulders normative joint movements.