In today’s blog post our Oakville physiotherapist at our Oakville Physiotherapy clinic will be discussing the topic of Thoracic Outlet Syndrome. First we will define the injury, explain the clinically relevant anatomy of the impairment, the three main types of compression in the thoracic outlet region, the etiology and differential diagnosis, signs and symptoms and management of the condition.
Since Covid we have been seeing a lot more TOS our our clinic. Computer posture and too much cell phone seems to be the culprit. Think you have TOS, get in today!
What is Thoracic Outlet Syndrome?
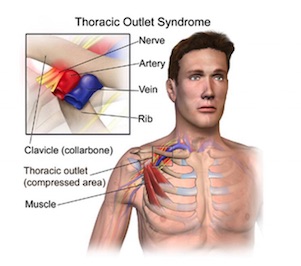
The injury thoracic outlet syndrome simply describes the compression of either the nerve or vascular (blood) structures as they pass through the ‘thoracic outlet’ of the body. 50-95% of patients diagnosed with thoracic outlet syndrome respond well to conservative management with their Oakville physiotherapist.
Usually it is an insidious onset that brings on the condition, which becomes progressively worse over time. Females are more susceptible to the injury then men at a 4 to 1 ratio, specifically middle-aged females as seen in the present literature. The injury may be caused by repetitive activities, trauma, and congenital anomalies or may occur idiopathically, meaning its origin is unknown.
Also, you should be aware that there are many synonymous terms for thoracic outlet syndrome. Therefore if you hear any of the following terms, be aware that it is simply the same injury stated in a different form and not multiple injuries. These terms are, but not limited to cervical rib syndrome, scalenus anticus syndrome, costoclavicular syndrome, hyperabduction syndrome, pectoralis minor syndrome, brachiocephalic syndrome, thoracic inlet syndrome, nocturnal paresthetic brachialgia, effort vein thrombosis, compression neuropathy of the brachial plexus, and vasculopathy of the brachial plexus.
Read More About Thoracic Outlet Syndrome Here
Anatomy of TOS
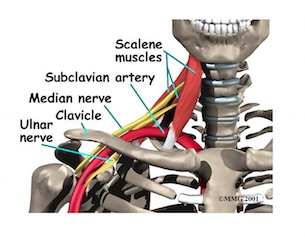
Now that we’ve confused you with what seems like a completely different language in regards to the synonymous terms, it’s time to understand the anatomy of thoracic outlet syndrome. Think of the injury as a triangle. The base of the triangle is the first rib, the right side of the triangle is anterior scalene muscle and the left boarder of the triangle is the middle scalene muscle.
The contents within this triangle are the brachial plexus, the subclavian artery. Therefore, compression of one of or multiple components of these three structures is what is known as thoracic outlet syndrome. Recognize that the brachial plexus is a series of different nerves exiting from the neck, and both the subclavian vein and artery is blood supply.
Therefore thoracic outlet syndrome is a neurovascular injury in nature. However, the majority of clinically relevant thoracic outlet injuries are neurological in nature and account for roughly 90% of all cases of thoracic outlet syndrome.
Types of Compression in the Thoracic Outlet
Scalene Triangle Compression
The most common area of compression is in the ‘scalene triangle’, which we described above. Due to tight scalenes, muscle spasm, muscle hypertrophy, anomalous fibromuscular bands or the presence of a cervical rib may cause this type of compression. The ‘cervical rib’ is seen in very few individuals and is an additional rib, which lies on top of the first rib.
Therefore, if you were born with an additional rib, the space of your ‘triangle’ has shrunk in nature, as your base would be heightened, therefore increasing the likelihood of compression to the brachial plexus or subclavian artery. Also, the dimensions of the triangle may be reduced if you extend your neck backwards or rotate your neck to the side of compression. These postural positions or positions which may occur from trauma may magnify this type of thoracic outlet injury.
First Rib Compression
The second type of compression is best understood as a sandwich. Imagine that the top piece of bread is the clavicle, your collarbone, and the bottom piece of bread is your first rib. Most often carrying a heavier load over your shoulders, such as a heavy backpack, causes this type of thoracic outlet syndrome. This type of compression may be reduced in sized by depression of the clavicle, retraction of the shoulders or extended your neck backwards.
The contents of this ‘sandwich’ are your subclavian artery and subclavian vein, therefore making this type of compression vascular in nature. At Glen Abbey physiotherapy we rarely see this type of compression, as the majority of all thoracic outlets are neural in nature.
Subclavian Compression
The third type of compression is called infraclavicular, meaning underneath the clavicle. On the front part of your shoulder there is a bone called your coracoid process, it almost looks like a bent finger, a muscle called pectoralis minor attaches onto it and acts like a sling that moves down and compresses the trunk of the brachial plexus against one of the ribs underneath it.
Therefore this type of compression is neural in nature and can be made worse by compression of your arm when it is fully raised away from your side in abduction and with slight lateral rotation.
Where Does TOS Come From?
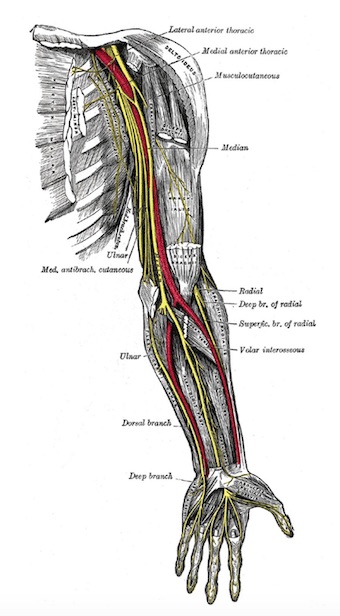
So now that we have an understanding of the three types of compression that may be seen with thoracic outlet syndrome, its time to understand the why. The different etiologies of the injury are the cervical rib, an elevated first rib, a larger first thoracic rib, hypertrophic scalene musculature, malunion of previously fractures clavicle, a pancoast tumor in the apex of the lung, an enlarged transverse process of the seventh cervical vertebrae, poor posture, trauma, exostosis and dislocation of the humeral head under the acromion. There are a fair number of differential diagnosis’ seen in thoracic outlet syndrome, meaning that although you may have signs and symptoms of the injury these injuries may be the true root cause: ulnar nerve compression, median nerve compression, cervical spondylosis, progressive muscular atrophy, myofascial trigger points, double crush syndrome and visceral causes.
Symptoms of TOS
There are numerous different symptoms that patients complain of at Glen Abbey Physiotherapy when working with their physiotherapist and team. Patients usually state that there is a radiating pain from the neck into the shoulder and down the arm, which is made worse by elevating their upper limbs. You may notice paraesthesia radiating down the arm, meaning numbness, tingling, burning pain. Pins and needles early in the morning beginning into the hand or forearm and move centrally up the arm and toward the neck as the day goes on is another symptom commonly seen in neural thoracic outlet syndromes. Your upper limb may feel heavy or weak in nature and tire easily as there would be a lower neural supply to the muscles innervated by your brachial plexus. Common vascular symptoms of patients with compression to their subclavian vein or artery are rapid fatigue and numbness of the arm in prolonged arm above head movements, lower temperature in arm, lacking pulse in the affected hand, cold swollen, glossy, discolored appearance of hand after exercising and there may be tenderness over the anatomical course of the subclavian artery or vein.
Signs of Thoracic Outlet Syndrome
When conducting a detail assessment of the patient at Glen Abbey Physiotherapy, we recognize pertinent signs, which help us diagnose a thoracic outlet syndrome. We may find tight scalene or pectoralis minor musculature, an alternation in your respiratory pattern, restricted accessory movements in your neck and cervical thoracic region of your spine, myotomal weakness with compression of the brachial plexus, positive orthopedic tests, muscle atrophy, signs of sympathetic involvement, the presence of a cervical rib seen on x-ray, positive nerve conduction studies, Doppler studies to reveal vascular involvement and a difference in blood pressure from the left and right arms. Any combination of these findings may lead us to believe a thoracic outlet syndrome may be the root cause of your injury or impairment.
Learn More About Symptoms of Thoracic Outlet Syndrome
Treatment for Thoracic Outlet Syndrome
Physiotherapy Treatment
 Physiotherapy Treatment
Physiotherapy TreatmentOnce a correct diagnosis is achieved, your physiotherapist and team will work with you to help correct, manage and prevent the injury from progressing and affecting your activities of daily living, sports, hobbies, work and everyday motions. We will prescribe the necessary exercises to decrease the amount of compression, utilize manual techniques to help facilitate joint movements, muscle releases and neural flow. Ice, heat, taping techniques, IFC, shockwave, ultrasound or acupuncture may all be additional modalities that your physiotherapist may utilize to help manage the present condition. Most of all your team at Glen Abbey Physiotherapy will help educate you about the condition and what you can do during your every day conduct to help reduce compressive forces to help alleviate your signs and symptoms, including at home stretches and exercises.
Acupuncture Treatment For Thoracic Outlet Syndrome
As discussed above, Thoracic Outlet Syndrome can originate from a number of sources. Acupuncture is an excellent option in treating thoracic outlet originating from tight muscles in the neck and causing nerve symptoms down the arm. Acupuncture is designed to affect the nerves, and can help calm down nerve-related symptoms. Dr. Jenn would target points in the neck, shoulder, elbow and hand to alleviate symptoms release muscle tension. Acupuncture is pain-free, effective and long-lasting.
If you or anyone you know may be suffering from thoracic outlet syndrome or you believe thoracic outlet syndrome may be the root cause to your signs and
symptoms, please visit us at Glen Abbey Physiotherapy and our physiotherapist and team would be happy to help you on your road to recovery.